INTRODUCTIONThe present study aims to evaluate the epidemiological profile of the 277 patients who suffered facial fractures and were treated at the Hospital do Trabalhador in Curitiba in the state of Parana, in 2010, with an emphasis on variables such as gender, age, cause, and anatomical sites of fractures, and compared with clinical findings of other studies in the literature.
Maxillofacial trauma can be considered as a devastating assault found in trauma centers because of the emotional consequences and the possibility of deformity, in addition to its economic impact on a healthcare system (1).
A maxillofacial injury involves not only the soft tissues and bones but also, by extension, can affect the brain, eyes, sinuses, and teeth.
Therefore, it is a trauma of a multidisciplinary approach, involving mainly the specialties of otolaryngology, ophthalmology, plastic surgery, maxillofacial, and neurosurgery (6).
Severe facial injuries may, in addition to psychological disorders, result in decreased productivity due to visual loss and damage during swallowing and phonation, increasing the costs arising from the trauma. The group most affected, men of working age, commonly found in many studies, partly explains the impact on productivity (2).
In the last 4 decades, the incidence of facial trauma has increased, mainly due to increased traffic accidents and urban violence, especially in young individuals (21). They are very common in emergency rooms around the world and assume a prominent role in the care to polytrauma patients.
The maxillofacial region is very prone to injury because of its prominence and little protection in the region. Further, it is the first area of attack in cases of interpersonal violence (5).
Today the association of alcohol, drugs, car driving, and increased urban violence are increasingly present as causal factors of facial trauma, and what is worse, increasing its complexity (7).
The medical literature is rich in epidemiological studies related to trauma and facial fractures. However, the epidemiology of craniofacial fractures can vary in type, frequency, severity, and cause, depending on the medical center studied and the period considered (3), because many factors influence the cause of maxillofacial injuries around the world, for example, cultural, economic, social, religious and geographical factors (4).
Therefore, epidemiological studies focused on facial injuries are of great interest as to the knowledge of the occurrence and quantity and severity of presentation, allowing the adoption of preventive measures for its control and management of patients.
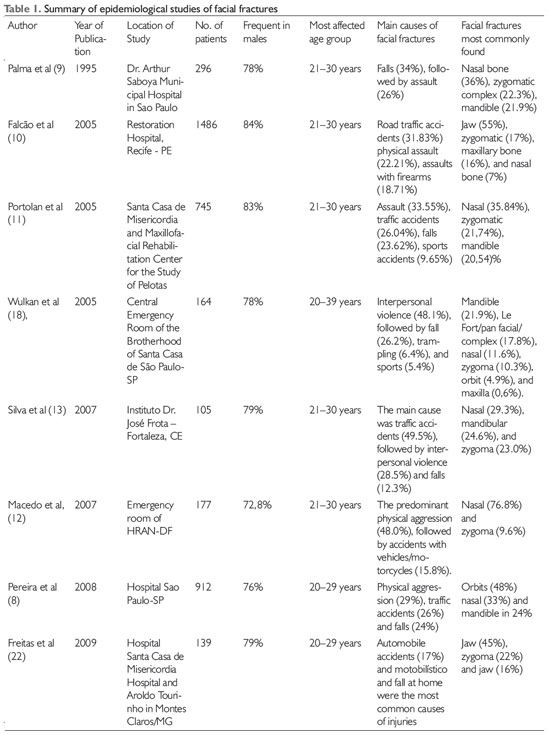
REVIEWThe medical literature is rich in epidemiological studies related to trauma and facial fractures. TABLE 1 shows the summary of several epidemiological studies of facial fractures in the literature in several cities. The table was divided according to the author, publication year, study site, number of patients suffering from facial fractures, male prevalence, age more acomentida, main causes of fractures and other broken facial bones.
METHODWe conducted a non-randomized retrospective study, of 277 patients with confirmed facial fractures diagnosed on radiographs and/or computed tomography, from the Otolaryngology Service at the Hospital do Trabalhador (HT) located in the city of Curitiba in Paraná during the year 2010.
The study included all patients treated at the Emergency Room of HT, attended by the Department of Otolaryngology, who were victims of facial trauma in the period from January 1 to December 31. We prepared a protocol for data collection performed by analysis of records and records of emergency in the sector of the medical file of the HT. This protocol included the following variables: medical record number, patient name, age, sex, origin, birth date, location of facial fracture, and cause.
The cause of the fractures was studied according to: motor vehicle crashes (combinations of collisions with cars, motorcycles, trucks/buses, and others), fall/bicycle accident, interpersonal violence with or without a firearm, drops own height or level falls, fractures arising from sports practices and impact/collisions with objects from accidental causes.
The locations of the fractures were classified into facial: fractures of the nasal bone, mandible, orbital, maxillary, frontal, zygomatic bone fractures, and Le Fort I, II, or III.
Data were analyzed with the aid of Microsoft Office Excel® 2007.
This research project was approved by the Ethics Committee of Hospital do Trabalhador.
RESULTSOf the 277 patients treated in 2010 evaluated in this study, 207 were male (74.72%) and 70 female (25.27%); the male to female ration was 3:1 (Figure 1). The patients' ages ranged from 1 to 79 years with a mean of 33.57 years.
The most affected age group was 20 to 39 years with 44.03% (Figure 2). The extremes of age, younger than 10 years and older than 70 years, accounted for respectively 13 (4.69%) and 8 (2.88%) patients.
The merits, 88.44% were residents of the city of Curitiba, 10.83% of the Metropolitan Region of Curitiba, and 0.72% from the interior the State of Paraná.
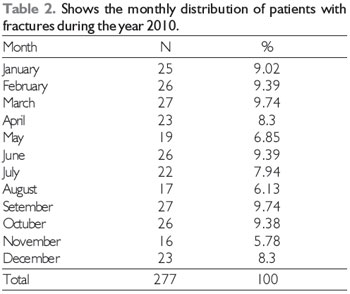
The number of patients treated per month ranged from 16 to 27, average of 23, September being the month with the highest number of visits (Table 2).
Regarding occupation, 55.23% had a professional activity, 16.96% were students, 5.77% were dependents, 5.41% were retirees, and 16.60% were unemployed or had indeterminate profession.
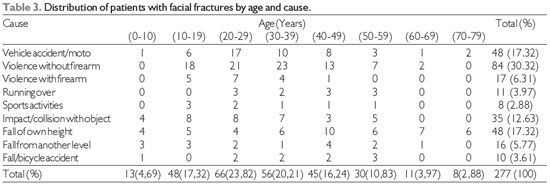
Regarding the cause of facial fractures, our chart review showed that the cause of fractures was interpersonal violence without firearm in 84 (30.32%) cases, interpersonal violence with a firearm in 17 (6.31%), motor vehicle accidents (car, truck, bus, motorcycle) in 48 (17.32%), injuries while walking in 11 (3.97%), from falls from a height in 48 (17.32%), due to drop in level in 16 (5.77%), due to impact/collisions with objects in 35 (12.63%), fall/bicycle accidents in 10 (3.61%), and sports injuries in 8 (2.88%) (Table 3).
The etiologic distribution by age showed a prevalence of violence without firearm in all age groups from 10 to 59, with a peak incidence in the age group 30-39 years with 41%. Falls from height predominated in the age groups 0-10 and 60-79, representing 57.9% of the causes of facial fractures in the latter. The motor vehicle crashes were the second most common cause in the age group 20-39 years with 22.13% of cases (Table 3). The motorcycles were involved in 47% of automobile accidents.
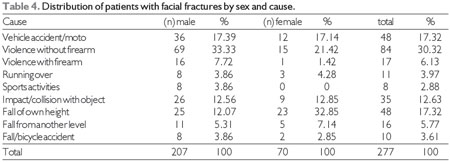
Regarding the cause and gender, falls from height were the main cause of facial fractures in women, corresponding to 23 (32.85%) cases in females followed by violence without firearm in 15 (21.42%) cases, and third, vehicle accidents with 12 (17.14%) cases. In the males, the main cause was violence without firearm in 69 (33.33%) cases, followed by motor vehicle accidents in 36 (17.39%), and third, by impact/collision with objects in 26 (12.56%) cases (Table 4 and Figure 3).
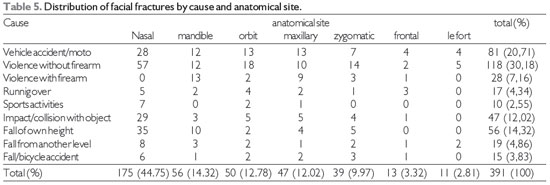
Patients had a total of 391 facial fractures, which were isolated in 205 (74%) cases and associated with 2 or more locations in 72 (26%). The nasal region was most affected, with 175 (44.75%) cases. Mandibular fracture was the second most common, found in 56 (14.32) cases, followed by the orbit with 50 (12.78%). Fracture of the maxilla was the fourth most frequent with 47 (12.02%), followed by the zygomatic bone with 39 (9.97). The more complex fractures Le Fort I, II, and III corresponded to 11 (2.81%) cases (Figure 4).
Table 5 Shows the distribution of fractures by cause and anatomic site of fracture.
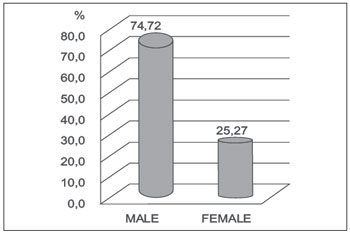
Figure 1. Distribution of patients with facial fractures according to sex in percentage (n = 277).
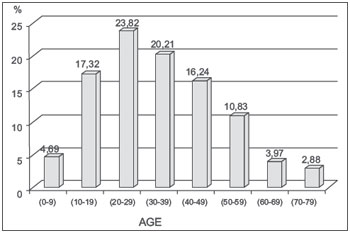
Figure 2. Distribution of patients with facial fractures according to age in percent (n = 277).
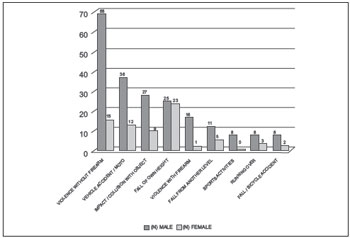
Figure 3. Distribution of patients with facial fractures by cause and gender (n = 277).
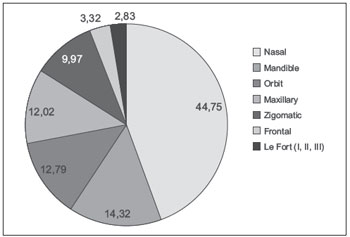
Figure 4. Distribution of fractures by anatomic location.
The face is susceptible to a variety of possible traumas, and it is important to note that aggression between facial injuries, especially fractures, plays a major role in emergency care worldwide.
Our study revealed a predominance of male patients with facial fractures corresponding to 74.72%, a 3:1 ratio, compatible with the literature including Palma et al, 78%, Falcon et al (10) , 84%, and Macedo et al, 72.8%. This higher incidence in males may be linked to cultural and social factors, considering that the males represent most of the economically active population, exhibit more abuse of alcohol and drugs, practice more contact sports, are involved in the majority in traffic, and thus are more exposed to the factors responsible for facial injuries. However, the incidence of trauma among women has increased in recent years due to the increased participation of women in the commercial workforce (16,17,18).
The patients' ages ranged from 1 to 79 years with a mean of 33.57 years. The most affected age group was 20 to 29 years, with 23.82% of cases. The age group also is in agreement with the findings of other authors such as Silva et al (13). The age group of 21-30 years in their study corresponds to 36.2% of cases. This is because young people are more prone to violence and psycosocioeconomic urban conflicts (13). It is understandable that violence occurs more among young people by their restlessness and risk taking behaviors, including traffic risks influenced by extremely fast behavioral and moral changes (16). At the extremes of age, patients younger than 10 years and older than 70 years accounted for respectively 13 (4.69%) and 8 (2.88%) patients, consistent with the literature findings (6-12) There are studies that show low incidence of facial trauma in children and the elderly due to the attention of family, stay at home, and care of children, as well as the characteristics of aging such as lessened social activity and sport, leaving little infrequently, and usually accompanied when they do. (14,15).
With regard to professional activity, our study showed that 55.23% had jobs and 16.96% were students, similar to studies by Macedo et al (12) JCM Junior et al in 2010 (6), and Brazil et al 2006 (16 ), the latter, which showed 60.5% of patients and 16.9% economically active students. This presents a problem because it is the predominant socioeconomically productive group.
Regarding the cause of facial fractures, our study showed the main causative agent of facial fractures was interpersonal violence without firearm with 84 (30.32%), and the second leading cause motor vehicle accidents (car, truck, bus, motorcycle) with 48 (17.32%) cases, as well as falls from height with the same values. These data are compatible with the current literature, which shows a growing share of violence as a cause of facial fractures, surpassing automobile accidents. This confirms the tendency of most recent national studies to show an increased incidence of interpersonal violence and suggest that this is the main cause in facial trauma (6,8,12,18). This is mainly due to an increase in urban violence and a drop in severity of motor vehicle accidents due to public policies aimed at greater control speeding on the roads and encouraging the use of seat belts. Moreover, the ban on drunk driving and the introduction of air bags and side protection bars have decreased the incidence of facial fractures, as well as the complexity (17,20). However, it calls attention to the involvement of 47% of motorcycles in traffic accidents, owing to the fact that unsafe vehicle speed abuse is practiced on the streets and that these vehicles are increasingly used because they are a means of low-cost transport.
Injurt from falls dominated as the cause in people aged under 10 and over 60, As these are extremes of age, because locomotion and balance are directly proportional to age. The consciousness of appearance of the face and its social importance increases with age (during a fall, older children and adults consider to protect the face) (14,15). In the case of elderly physiological mechanisms such as altered proprioception, weakness, tremor, and decreased reflexes facilitate queda. Infecção urinary tract and lung, and alcohol are also referred to (18).
With the number and location of the fracture, a total of 391 facial fractures, being isolated in 205 (74%) cases, and 2 or more locations associated in 72 (26%). Fractures are isolated mainly caused by low-energy trauma and interpersonal aggression. The nasal region was the most affected 44.75% of cases. Mandibular fracture was the second most commonly found in 14.32% cases, followed by 12.78% of the fractures in the orbit; maxilla fracture was the fourth most frequent with 12.02% followed by the zygomatic bone with 9.97%. The more complex fractures Le Fort I, II, and III accounted 2.81% of cases. These data differ widely in the literature, which show that in many cases, the jaw is the main bone fractured because it is the only mobile bone of the face and thus is more vulnerable to strong impact and fracture (10,16). On the other hand, studies like those by Silva et al. (13) and Leite et al. (19) corroborate our data demonstrating the nasal bone as the main fractured bones due to its prominent position, location on the mid-face, as well as the thin structures of the bones that constitute it.
The most serious fractures such as Le Fort occurred in 2.81% of cases. Of the total number of Le Fort fractures, 45% were due to interpersonal violence without firearm; trauma and morbidity are high in this type of fractures, and the cause is easily avoidable.
CONCLUSIONSFacial fractures are commonly reported in emergency departments worldwide. They are major causes of morbidity and socioeconomic prejudicial. The study of the epidemiology of facial trauma is important for the studying the cause and effects of facial trauma, assist in the initial care of these patients, and publishing preventive policies.
Our study showed that males are more affected and the main causes of facial fractures are assaults, motor vehicle accidents, and falls. They are more common in young patients aged 20-29 years followed by those aged 30-39 years. In the vast majority are isolated fractures and the most affected bone is the nose, followed by the lower jaw, orbit, maxillary, and zygomatic.
For the prevention of facial fractures, we must bear in mind the respect for traffic laws and routinely use seatbelts and helmets. Furthermore, the incidence of facial fractures can be reduced by strategies for dealing with falls in children and the elderly, avoiding hostile situations, and creating stricter laws and public policies to reduce traffic accidents and reduce interpersonal violence.
REFERENCES1. Sastry SM, Sastry CM, Paul BK, Bain L, Champion HR. Leading causes of facial trauma in the major trauma outcome study. Plast Reconstr Surg. 1995, 95:196-7.
2. Girotto JA, Mackenzie E, Fowler C, Redett R, Robertson B, Manson PN. Long-term physical impairment and functional outcomes after complex facial fractures. Plast Reconstr Surg. 2001;108(2):312-27.
3, Subhashraj K,Nandakumar N, Ravindran C. Review of maxillofacial injuries in Chennai, India: A study of 2748 cases. British Journal of Oral and Maxillofacial Surgery. 2007;45: 637-639.
4. Gabrielli MAC, Gabrielli MFR, Marcantonio E, Hochuli-Vieira E. Fixation of mandibular fractures with 2.0-mm miniplates: review of 191 cases. J Oral Maxillofac Surg. 2003;61(4):430-6.
5. Gandhi S, Ranganathan LK, Solanki M, Mathew GC, Singh I, Bither S. Pattern of maxillofacial fractures in northern India. a 4-year retrospective study of 718 patients.Dental Traumatology 2011; 27: 257-262;
6. Junior JCM, Keim FS, Helena ETS. Aspectos Epidemiológicos dos Pacientes com Traumas Maxilofaciais Operados no Hospital Geral de Blumenau, SC de 2004 a 2009. Arq. Int. Otorrinolaringol. 2010;14(2):192-198
7. Montovanijc JC, Campos LMP, Gomes MA, Moraes VRS, Ferreira FD, Nogueira EA. Etiologia e incidência das fraturas faciais em adultos e crianças: experiência em 513casos. Rev Bras Otorrinolaringol 2006;72(2):235-41
8. Pereira MD, Kreniski T, Santos RA, Ferreira LM. Trauma craniofacial: perfil epidemiológico de 1223 fraturas atendidas entre 1999 e 2005 no Hospital São Paulo - UNIFESP-EPM Rev Soc Bras Cir Craniomaxilofac 2008; 11(2): 47-50
9. Palma VC, Luz JGC, Correia FAS. Frequência de fraturas faciais em pacientes atendidos num serviço hospitalar.Rev Odontol Univ São Paulo. 1995; 9(2):121-6.
10. Falcão MFL, Segundo AVL, Silveira MMF. Estudo epidemiológico de 1758 fraturas faciais tratadas no Hospital da Restauração, Recife/PE. Rev Bras Cir Traumatol Buco-Maxilo-Fac. 2005;5(3):65-72.
11. Portolan M, Torriani M. Estudo de prevalência das fraturas bucomaxilofaciais na região de Pelotas. Rev Odonto Ciênc. 2005;20:47.
12. Macedo JLS, Camargo LM, Almeida PF, Rosa SC. Perfil epidemiológico do trauma de face dos pacientes atendido no pronto socorro de um hospital público. Rev. Col. Bras. Cir. 2008;35(1):009-013.
13. Silva JJL, Lima AAAS, Torres SM. Fraturas de face: análise de 105 casos. Rev Soc Bras Cir Craniomaxilofac 2007;10(2): 41-50
14. Haug RH, and Foss J. Maxillofacial injuries in the pediatric patient. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2000;90:126-34
15. Lucht UA. A prospective study of accidental falls and resulting injuries in the home among elderly people. Acta Soc Med Scand. 1971, 2:105-9.
16. Brasileiro BF, Passeri LA, Epidemiological analysis of maxillofacial fractures in Brazil: A 5-year prospective study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 12006;102:28-34.
17. Montovani JC, Campos LMP, Gomes MA, Moraes VRS, Ferreira FD, Nogueira EA. Etiologia e incidência das fraturas faciais em adultos e crianças: experiência em 513 casos. Rev Bras Otorrinolaringol. 2006;72:235-41.
18. Wulkan M, Júnior JGP, Botter DA. Epidemiologia do trauma facial. Rev Assoc Med Bras. 2005;51(5):290-5.
19. Segundo AVL, Campos MVS, Vasconcelos BCE. Perfil epidemiológico de pacientes portadores de fraturas faciais. Rev. Ciênc. Méd., Campinas 2005;14(4):345-350.
20. Barros TE, Campolongo GD, Zanluqui T, Duarte D. Facial trauma in the largest city in Latin America, São Paulo, 15 years after the enactment of the compulsory seat belt law. Clinics (Sao Paulo). 2010;65(10):1043-7.
21. Cardozo DD, Bergoli RD, Torriani MA. Levantamento epidemiológico dos traumatismos faciais em pacientes pediátricos assistidos no pronto socorro municipal de Pelotas. Trabalho de Conclusão de Curso - Faculdade de Odontologia, Universidade Federal de Pelotas, Pelotas, 2004.
22. Freitas DA, Caldeira LV, Pereira ZM, Silva AM, Freitas VA, Antunes SLNOC. Estudo epidemiológico das fraturas faciais ocorridas na cidade de Montes Claros/MG. Rev Bras Cir Cabeça Pescoço 2009;38(2):113-5.
1) Medical. Medical Resident.
2) Master. Chief of the Skull Maxillofacial Surgery Service of Otorhinolaryngology UFPR.
3) Postgraduate. Skull Maxillofacial Surgeon in the Department of Otorhinolaryngology, Hospital do Trabalhador-PR.
4) Graduation. Medical.
5) Academic. Doctoral student in the 6th year medical UFPR.
Institution: Hospital do Trabalhador de Curitiba / PR. Curitiba / PR - Brazil. Mailing address: Renier Barreto Arrais Ykeda - Rua Augusto Zibarth, 1081 - Uberaba, 81560-360 - Curitiba / PR - Brazil - Telephone: (+55 41) 3360-6588 - E-mail: ykedabarreto@yahoo.com.br
Article received in March 3, 2012. Article approved in June 7, 2012.