INTRODUCTIONWith the objective to obtain an adequate evaluation of all vestibulocochlear system, the use of tests which evaluate the auditory processing has been shown a challenger instrument of clinical audiology (14).
Hearing losses and history of otitis can be risk indicators for auditory processing development, as well as for language development, speech and learning, as the literature has been established that children with history of recurrent otitis during the childhood tend to have significant differences on the performance of hearing perception, auditive memory, acquisition of oral language and scholar progress (4,16).
According to American Speech Hearing Association (2) (ASHA), auditory processing disorder (DPA) is a change in one or more mechanisms or processes of auditory system responsible for the conduct of sound localization and lateralization; auditory discrimination; auditory pattern recognition; temporal aspects of hearing, including resolution, masking, integration and temporal ordination; auditory performance in the presence of competitive signs and auditory performance with acoustic signs degraded.
By studying the relation among the recurrent otitis media, language and auditory processing, it was checked that the language and auditory processing in children with Otitis Media with Effusion (OME) presented results significantly worse than children that did not presented history (8). Many authors affirmed that children with recurrent otitis during the childhood tend to present significant differences on the auditory perception performance, auditory memory, oral language acquisition and scholar progress (4, 3, 20,29).
Other authors (23) who affirmed that, individuals with peripheral hearing loss probably will have impaired performance on test of auditory processing. However, it could be persons that, even presenting peripheral hearing loss (from light to moderate level), present normal auditory processing.
Cleft Palate (CP) is a result of malformation due to failures on development or in the maturation processes embryonic (1).
Several studies (10, 11, 21, 27) have emphasized peripheral hearing in the population with CP, being largely known to its high incidence of alterations in the middle ear, due to a faulty velotubal aeration mechanism . Thus, the media otitis and hearing losses of conductive type, usually bilateral, have figured as the most important pathologies in this population. These changes have as consequence a sensory deprivation, leading it to a risk indicator to changes in the auditory process development, language, speech, learning and cognitive potential of a child with CP.
However, studies show emerging (5, 7, 9, 17, and 18) over the hearing processing in children with CP.
The identification of difficulties of auditory verbal processing and non-verbal in preschool and school children has importance affirmed in academic foundations, maturational, psychological and economics. The premature identifications in children with limitations in the hearing processing skills reduce the time and other costs for intervention (15).
Considering that hearing losses and otologic complications can interfere in the maturation processe of central nervous system, this study had as objective to verify the performance of children with CP and with or without media otitis history in the evaluation of auditory processing.
METHODThis study was approved by the Ethics and Research Committee from institution where it was held, with protocol number 15/2001.
20 children of both genders regularly enrolled in a referral hospital for rehabilitation of craniofacial anomalies in the state of São Paulo participated in this study
The criteria of inclusion of the participants in this study were: have CP operated, being in the age group between 7 to 11 years old, do not present complaint and/ or superior airway infection in exam situation, do not present neurological disorder history, parents permit and the Term of Free and Clarified Consent signed.
The children formed two groups, divided according to the presence of not of otitis history:
-Group I (GI) - constituted of 10 children with CP with otitis history.
-Group II (GII) - constituted of 10 children with CP without otitis history.
It was performed comparing between the findings of the groups sampled (GI e o GII).
The auditory processing tests were selected considering the age group and hearing development.
The applied tests are divided in: diotic, monotic and dichotic.
The diotics tests (22) are tests where the same stimuli are presented simultaneously to both ears. They are: Sound Locate Test in 05 directions (right, left, behind, above and front) (22), Memory Tests for Verbal Sounds and Non-Verbal Sounds in sequence (22) and the Auditory Fusion Test - Revised - AFT-R (24) which is a procedure to measure the temporal processing skill, determining the length (in ms) in which the listener can detect a short break of silence between two tones, and report if he heard or not one or two tones.
The monotics tests (28) are tests in which different stimuli or not are presented simultaneously to the same ear, i.e., ipsilaterally. They are: Words and Phrases cith Ipsilateral Competitive Message Test - Pediatric Speech Intelligibility (PSI) in which verbal stimuli used are 10 phrases that are presented randomly, along with a competitive message, which must be identified by child indicating the figure that it represents, being the competitive message an infant story; the Speech in Noise Test with figures e with words (PSI with words) composed of 10 words which must be indentified through the figure that corresponds to the word listened can be performed with two competitive different messages ipsilaterally (white noise or an infant story); the Phrases Test with Ipsilateral Competitive Message (SSI) in which are used verbal stimuli composed of 10 synthetic third-order phrases and the competitive message is a Brazil history text.
The dichotic tests are composed of different stimuli simultaneously to both ears. The Dichotic Test with Competitive Non-Verbal Sounds (22) is performed with 03 environmental sounds (noise of thunder, church bell noise and a noise of door slamming) and three onomatopoeic sound (sound of cat meowing, barking dog and rooster crowing), that must be identified by indicating the figures that it represents. These sounds were combined among them and synchronized in time in order to form twelve pairs. In the Test Staggered Spondaic Word (SSW) (6) are used as verbal stimuli 160 words composed of two-syllable from Brazilian Portuguese and the Digits Dichotic Test (26) are constituted of 20 pairs of digits which represent two-syllables in Portuguese.
These tests were performed in acoustic cabinet through an two channels audiometer engaged to a CD player.
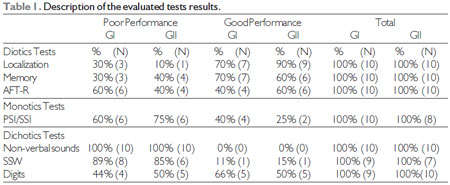
The results were analyzed and compared with normal standard proposed by each test, being classified as bad performance those which presented lower score than the normal and good performance the others.
It was performed descriptive statistical analysis of the groups according to the performance in each test, comparing the results of group I and group II.
RESULTSSome children that participated in this study could not perform all of the proposed and described tests in the methodology of this study, for not understanding the instruction to perform the test or presented articulatory problems. Thus, the Dichotic test was not performed in a child (GI), the test SSW was not performed in four children (1 GI e 3 GII) and the test SSI/PSI was not performed in two children (GII).
On Table 1 are described the tests results evaluated according to the children performance in the groups sampled.
DISCUSSIONBoth groups (GI e GII) presented bad performance in most of the tests. However, the population with otitis history (GI) presented worse results in auditory processing evaluation, if compared to the population without otitis history (GII).
It was observed that, regardless of the presence of otitis history in the first years, the population with lip and palate cleft presented considerable difficulties in the applied tests, indicating percentage change in both groups, being the otitis an aggravation of the situation.
Children without otitis history (GII) presented normal performance in dichotics tests, whereas, in other test, it was predominantly poor performance. The children with otitis history (GI) presented lower rates in normal performance, compared to GII, being more frequent poor performance in dichotics tests.
These data are consistent with literature found, given that in almost of the studies involve auditory processing and CP the evaluation results presente high rate of changes. (7,5).
Comparing the performance good and bad among evaluated children belonging to the same group, it was possible to conclude that the tests with more poor results were SSW and Non-Verbal Dichotic for GI. For GII, the tests PSI and SSI also presented high rate of poor performance, beyond of SSW and Dichotic Non-Verbal.
In children without CP and with suspect of hearing change there was a greater change on the dichotics tests results, specially the Dichotic of Digits and SSW, being these tests of high linguistic level made them to be more sensitive to identify changes in the auditory processing (12).
In relation to the test AFT-R, the performance changed rate of otitis history group (GI - 60%) was higher. It is known that a higher threshold of auditory fusion leads to a greater probability of temporal processing deficit and interference in speech perception (19).
The literature reports that children with FLP presents threshold of auditory fusion significantly greater than the children without this malformation (9). This fact can be justified by the high occurrence of otitis in population with CP.
Presence of otitis history during childhood can interfere in auditory skills development and in the perception of the distinctive features of speech, which may lead to phonological changes.
The presence of otitis history can cause greater prejudices in auditory skills of figure-ground and auditory closure, auditory memory and language (25).
The exact determination of the relation between media otitis and Auditory Processing Disorder has not been widely elucidated. It is necessary caution in the results interpretation and determination of other variables can be interfering as na etiology to Auditory Processing Disorder, like malnutrition, sociocultural environment with few stimuli, reducing motivation and the health state in general (30).
CONCLUSIONIt was observed that, regardless of the presence of otitis history in the first years, the population with CP presented important difficulties on the applied tests, indicating poor performance percentage in both of groups, being otitis an aggravation of the situation.
Thereby, it is suggested the auditory processing evaluation in the whole population with CP and not only in those who otitis are the risk indicators, so that to establish a large and complete study of rehabilitation, as the auditory processing difficulties can interfere on the language development and school performance.
BIBLIOGRAPHY REFERENCE1. Altmann EBC. Fissuras labiopalatinas. Carapicuíba: Pró-Fono; 1997.
2. American Speech-language-hearing Association (ASHA) - Central auditory processing: current status of research and implications for clinical practice. Am J Audiol. 1996, 5(2):41-54.
3. Asbjornsen A, Holmefjord A, Reisæter S, Moller P, Klausen O, Prytz B et al. Lasting auditory attention impairment after persistent middle ear infections: a dichotic listening study. Develop Med Child Neurol. 2000, 42(7):481-486.
4. Balbani APS, Montovani JC. Impacto das otites médias na aquisição da linguagem em crianças. J Pediatr. 2003, 79(5):391-6.
5. Beloni M, Santos MFC. Processamento auditivo em crianças com fissura labiopalatina não-sindrômica. In: Anais do 20º Encontro Internacional de Audiologia; 2005 abril: São Paulo, SP [em CD-ROM].
6. Borges ACLC. Dissílabos Alternados - SSW. In: Pereira LD, Schochat E. Processamento auditivo central: manual de avaliação. São Paulo: Lovise, p.169-178.
7. Boscariol M, André KD, Feniman MR. Crianças com fissura isolada de palato: desempenho nos testes de processamento auditivo. Braz J Otorhinolaryngol. 2009, 75(2):213-20.
8. Campbell N, Hugo R, Uys I, Hanekom J, Millard S. Early recurrent otitis media, language and central auditory processing in children. S Afr J Commun Disord. 1995, 42:73-84.
9. Cassab TV, Zorzetto NL. Teste da fusão auditiva-revisado (AFT-R) em crianças com fissura labiopalatina. ACTA ORL/Técnicas em Otorrinolaringologia. 2006, 24(4):272-76.
10. Feniman MR, Souza AG, Jorge JC, Lauris JRP. Achados otoscópicos e timpanométricos em lactentes com fissura labiopalatina. Rev Bras Otorrinolaringol. 2008, 74(2):248-52.
11. Gloudy S, Lott D, Canady J, Smith RJH. Conductive hearing loss and otopathology in cleft palate patients. Otolaryngology-Head and Neck Sugery. 2006,134(6):946-948.
12. Gonçales AS, Souza LB, Souza VMC. Avaliaçao do processamento auditivo:relato de experiência clínica. In: Aquino AMCM. Processamento Auditivo: eletrofisiologia e pscioacústica. São Paulo: Lovise, 2002.
13. Hall JW, Grose JH. Effect of otitis media witheffusion comodulation masking release in children. J Speech Hear Res. 1994, 37(6):1441-49.
14. Jacob LCB, Alvarenga KF, Zeigelboim BS. Avaliação audiológica do sistema nervoso auditivo central. Arq Int Otorrinolaringol. 2000, 4(4):144-51.
15. Kelly D. A rationale for screening for central auditory processing difficulties at the kindergarten and second-grade levels: considerations for the Speech-Language Pathologist. Disponível em: www.turtan.com.
16. Klausen O, Moller P, Holmefjord A, Reisaeter S, Asbjornsen A. Lasting effects of otitis media with effusion on language skills and listening performance. Acta Otolaryngol Suppl. 2000, 543:73-76.
17. Laasonen M, Haapanen ML, Mäenpää P, Pulkkinen J, Ranta R, Virsu V. Visual, Auditory, and Tactile Temporal Processing in Children With Oral Clefts. Journal of Craniofacial Surgery. 2004, 1(3):510-8.
18. Lemos ICC. Habilidade de Atenção Auditiva em Crianças de Sete Anos Com Fissura Labiopalatina: Estudo Comparativo. Tese, Bauru, 2007.
19. McCrosckey R, Keith RW. AFT-R: Auditory fusion test-revised. San Antonio, TX: Psychological Corporation, 1996.
20. Northern JL, Dows MP. Audição em crianças. São Paulo: Manole, 3 ed., 1989.
21. Pegoraro-Krook MI, Souza JCRD, Teles-Magalhães LC, Feniman MR. Intervenção Fonoaudiológica na Fissura Palatina. In: Ferreira LP, Beffi-Lopes DM, Limongi SCO. Tratado de Fonoaudiologia. São Paulo: Roca. 2004; p. 439-455.
22. Pereira LD. Temas Sobre o Desenvolvimento - Processamento Auditivo. 1993, (11):7-14.
23. Ramos CS, Pereira LD. Processamento auditivo e audiometria de altas freqüências em escolares de São Paulo. Pró-Fono Rev Atual Cient. 2005, 17(2):153-164.
24. Samelli AG, Schochat E. Processamento auditivo, resolução temporal e teste de detecção de GAP: revisão da literatura. Rev CEFAC. 2008, 10(3):369-377.
25. Santos MFC, Ziliotto KN, Monteiro VG, Hirata CHW, Pereira LD, Weckx LLM. Avaliação do Processamento Auditivo Central em Crianças Com e Sem Antecedentes de Otite Média. Rev Bras Otorrinolaringol. 2001, 67(4):448-54.
26. Santos, MFC. Processamento auditivo central: teste dicótico de dígitos em crianças e adultos normais. Tese, São Paulo, Universidade Federal de São Paulo Escola Paulista de Medicina de Medicina, 1998:198.
27. Souza D, Ninno CQMS, Borges GP, Silva TM, Miranda ES. Perfil audiológico de indivíduos operados de fissura de palato no Hospital da Baleia de Belo Horizonte. ACTA ORL/Técnicas em Otorrinolaringologia. 2006, 24(3):170-173.
28. Toniolo IMF, Rossi AG, Borges ACLC, Pereira LD. Processamento Auditivo: habilidade auditiva de memoria sequencial verbal e nao verbal em escolares. Rev Saúde. 1994, 20(3-4):11-22.
29. Wertzner HF, Oliveira MMF. Semelhanças entre sujeitos com distúrbio fonológico. Pró-Fono Revista de Atualização Científica. 2002, 14(2):143-152.
30. Mahon E. Processamento Auditivo Central e Otite Média. 1999. Centro de Especialização em Fonoaudiologia Clínica (CEFAC), Recife. Muscrito.
1) Speech Therapist. Master´s degree program at college Faculdade de Odontologia de Bauru -São Paulo University, Speech Therapist Field.
2) Mestre. Doutoranda em Saúde Coletiva pela FMB/UNESP.
3) Speech Therapist Graduated at Fonoaudióloga Graduada pelo Speech Therapy Course the FOB/USP.
4) Professor of the Department of Speech FOB/USP. Reasearch Sponsored by National Research Counsil - Conselho Nacional de Pesquisas (CNPq).
Institution: São Paulo University , Bauru Dentistry College, Speech Therapy Department, Speech Therapy Clinic. Bauru / SP - Brazil. Mailing address: Mariza Ribeiro Feniman - Alameda Dr. Octávio Pinheiro Brizolla, 9-75 - Vila Universitária - Bauru / SP - Brazil - Zip Code: 17012-901 - Telephone: (+55 14) 3235-8332 - E-mail: feniman@usp.br
Article received on 2011 March 17th. Article approved on 2011 July 21st.